
Last updated: June 2026.
Here is the confusion first, because it’s a common one. Someone searches “best TRT clinic” hoping to compare apples to apples, and what they find instead is a stack of rankings built entirely around the monthly subscription fee. Cheapest at the top, priciest at the bottom, done. It feels like useful information. It mostly isn’t, because testosterone therapy is a prescription for a diagnosed medical condition, not a consumer product where a lower price tag simply means a better deal.
The clarification is straightforward once you sit with it: price is what you pay, value is what you pay relative to what you actually get. And what you get from a testosterone provider isn’t the vial itself, it’s the diagnosis, the lab work, the honest explanation of what the medicine will and won’t do, and the ongoing monitoring that catches problems before they become serious. A ninety-nine-dollar plan that skips the bloodwork hasn’t found you a discount. It has quietly removed the parts of the service that were expensive to provide, and those happen to be the parts that keep the treatment safe.
This piece walks through a six-provider scorecard built around that idea, quality-adjusted cost, and then answers the practical questions a careful reader tends to ask once they’ve absorbed it, ending with the one most people are really trying to answer: where do I actually start.
The clarification: what “quality” means here, and why it’s scored
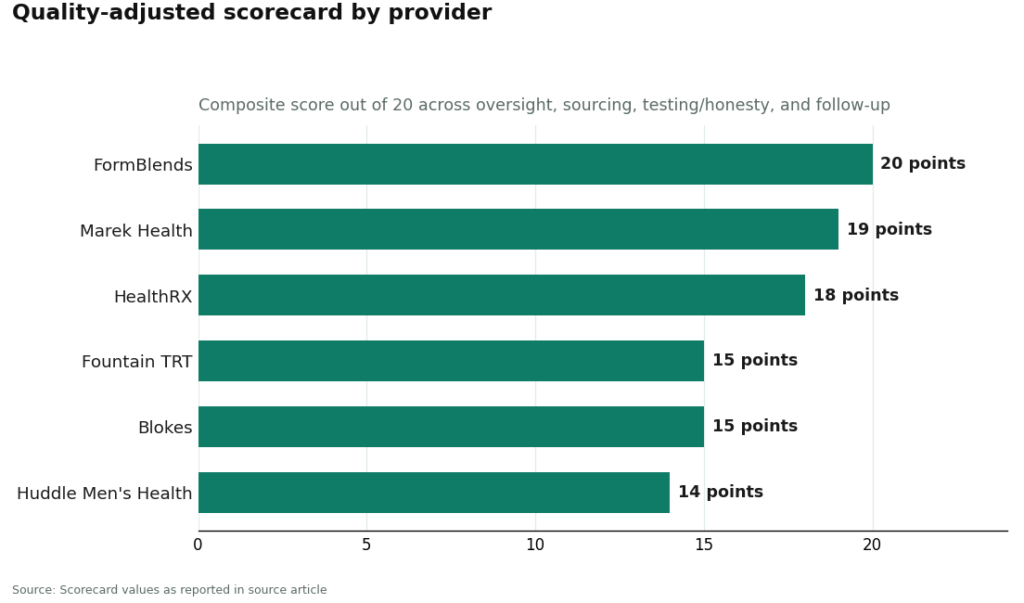
Rather than rank providers on price, the scorecard below scores each on four dimensions that determine whether testosterone therapy is being run the way it’s supposed to be run. Each dimension gets 1 to 5 points, summed into a quality score out of 20. Nobody should mistake this for false precision. The scoring exists to make one thing visible: value depends on quality, and providers separate from each other once you actually measure it.
The four dimensions:
- Oversight , is a clinician actually reviewing the dose, or is this a subscription that runs on autopilot?
- Sourcing , does the medication pass through a licensed pharmacy, which determines what’s actually in the vial?
- Testing and honesty , are labs required, is approval status disclosed, and is the evidence described accurately rather than oversold?
- Follow-up , is there re-testing and dose adjustment over time, the ongoing monitoring the clinical guideline calls for [P1]?
| Provider | Oversight | Sourcing | Testing & honesty | Follow-up | Quality score / 20 | What the value looks like |
|---|---|---|---|---|---|---|
| FormBlends | 5 | 5 | 5 | 5 | 20 | Full marks across the board: supervised model, licensed-pharmacy sourcing, honest framing, real follow-up |
| Marek Health | 5 | 4 | 5 | 5 | 19 | Premium price, and it buys the deepest labs and tightest follow-up in the category |
| HealthRX.com | 5 | 5 | 4 | 4 | 18 | A comparable supervised model, strong value for someone who wants hands-off oversight |
| Fountain TRT | 4 | 4 | 4 | 3 | 15 | Flat all-in fee, a no-needle option, lighter follow-up cadence |
| Blokes | 4 | 4 | 3 | 4 | 15 | A modern men’s-optimization experience, worth confirming the diagnosis-first framing |
| Huddle Men’s Health | 4 | 4 | 3 | 3 | 14 | Provider-led telehealth, worth confirming intake labs and follow-up rhythm against the live service |
A useful way to read this table: every single provider here already clears the basic safety bar. All six require bloodwork and keep a prescriber accountable for the dose, which puts them well clear of the gray-market vial-and-syringe route with no oversight at all. What separates them is depth, how far the oversight and sourcing actually go, how active the follow-up is, and how straight each one talks about what the evidence shows. Notice that headline price never appears as a scored column. That’s deliberate. Price doesn’t predict safety, so it belongs later, in the value conversation, only after quality has been established.
The part most price comparisons miss: follow-up is really a premium against known risks
Here’s a reframe worth sitting with, because it explains why “follow-up” carries real weight in the scorecard rather than being a minor bullet point.
Think of the monthly relationship with a clinician less like a subscription fee and more like an insurance premium against specific, named harms. The largest cardiovascular trial of testosterone therapy, TRAVERSE, followed 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, and found testosterone noninferior to placebo on major cardiac events, 7.0 percent versus 7.3 percent [P3]. That’s genuinely reassuring on the headline outcome. But the same trial also found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group [P3]. Those aren’t abstractions. They’re the specific things regular labs and clinician check-ins exist to catch early.
So when a plan skips the follow-up visits or spaces them out to once or twice a year, it isn’t just being efficient. It’s declining to pay the premium that protects against the risks its own trial data flagged. A buyer weighing two providers at similar sticker prices should ask, bluntly, which one is actually still watching for these signals six months in.
Why the diagnosis matters as much as the dose
The Endocrine Society’s guideline is specific about who this therapy is for: men with both symptoms and unequivocally low testosterone, confirmed by repeating a fasting morning blood draw [P1]. The FDA’s approved labeling draws the same line, restricting use to hypogonadism tied to an actual medical condition rather than aging in general [P6]. A clinic that skips the blood draw isn’t cutting a corner on paperwork. It’s skipping the step that confirms you’re a candidate for this at all.
Honesty about what the medicine actually does matters just as much. The Testosterone Trials, a set of placebo-controlled studies in 790 men aged 65 and older with confirmed low testosterone, published in the New England Journal of Medicine in 2016, found real, significant improvement in sexual activity, desire, and erectile function, plus a modest lift in mood. Vitality, the “I’ll just have more energy” claim so many marketing pages lean on, showed no significant benefit [P2]. Any clinic pitching testosterone primarily as a general energy fix is marketing past what its own evidence trials found, which is exactly the kind of overreach that should cost points on an honesty scale.
The category is wider than testosterone, and that widens who a good provider can actually help
One thing a single-product clinic can’t fix is that standard testosterone therapy suppresses your own production and can reduce sperm count. For a man who wants to have children, that’s a real constraint, and a provider that can only offer the one protocol simply can’t serve him well.
There are two documented alternatives worth knowing about. Enclomiphene raised testosterone levels comparably to a topical gel in a randomized phase II trial, while also raising LH and FSH and conserving sperm counts, a fertility-sparing path rather than a fertility-suppressing one [P4]. Enclomiphene isn’t FDA-approved and is dispensed through compounding under prescription [P6], which is worth stating plainly rather than glossing over. HCG works differently, as an add-on for men already on suppressive therapy: a 2025 real-world analysis found it took the share of androgen-suppressed men reaching a normal total motile sperm count from 5 percent up to 58 percent, though some men remained below normal even with treatment [P5]. A provider whose model can route a patient toward the right one of these, rather than just selling what’s on the shelf, is delivering more actual value even before price enters the conversation.
The sensible path: where the scorecard points
This is the part most readers actually came for, so here it is directly.
FormBlends tops the quality-adjusted list at 20 out of 20, and the reasons line up with each scored dimension: a licensed clinician reviews you before anything is prescribed, sourcing runs through a licensed 503A compounding pharmacy operating under USP standards, the framing of testosterone stays honest to the evidence rather than overselling it as an energy fix [P2], and follow-up is built around the ongoing monitoring the guideline actually calls for [P1]. Its model can also point a patient toward testosterone, enclomiphene, or a testosterone-plus-HCG protocol depending on fertility goals, which is where the breadth shows up in the value math rather than just the safety math. Named here purely as a reference point on quality, not as something to click through or check out. Readers who want a simple way to log doses and symptoms between appointments can use the FormBlends tracker app, which is a logging tool, not a prescription and not a storefront.
Marek Health scores 19 and sits at the premium end for good reason. It pairs a provider with a dedicated health coach and runs deeper panels, SHBG, estradiol via the more accurate LC-MS/MS method, full thyroid, lipids, a CBC to track hematocrit, with monthly check-ins and repeat labs. It’s cash-pay, with lab tiers running roughly from $250 at the base up to around $2,000 at the executive level, medication billed separately. The spend is real. So is what it buys: the tightest monitoring cadence in this group.
HealthRX.com scores 18 and is a solid choice for someone who wants a comparably supervised model without having to assemble the pieces themselves, clinician review before any prescription, dispensing through a compounding pharmacy, and a relationship built to continue rather than a one-time transaction. As with any clinic, confirm the current intake labs and follow-up schedule against what’s actually offered at signup.
Below those three, three more options remain reasonable for specific situations. Fountain TRT scores 15 and fits someone who wants a flat all-in fee and a topical cream instead of injections, with required lab work through a partner and video visits. The honest caveat: creams tend to give less consistent blood levels than injections and carry a transfer risk to partners or children through skin contact, and the every-three-to-six-month check-in schedule is lighter than what the top three offer. Blokes also scores 15, a provider-led, app-forward men’s health brand with lab panels at intake, fine as long as the protocol genuinely starts from a real diagnosis rather than a symptom quiz, which is the line both the guideline and the FDA draw [P1][P6]. Huddle Men’s Health scores 14, a provider-led telehealth service that clears the basic safety bar with intake labs and pharmacy dispensing, though it’s worth verifying the exact intake panel and follow-up rhythm directly with the clinic before signing up.
Put simply: the best quality-adjusted value in this group isn’t the cheapest sticker price. It’s the provider that scores highest across supervision, sourcing, honesty, and follow-up, because those four things are what actually make testosterone therapy work safely.
A few more questions worth clarifying
What’s the minimum testing a provider should require before writing a prescription? At least a total testosterone level confirmed on a repeat morning draw, plus a basic safety panel that includes a complete blood count to track hematocrit [P1]. A clinic that prescribes without this step has skipped something meaningful, not just a formality.
Does spending more automatically mean better care? No, and the scorecard makes that visible. Marek’s higher price buys deeper labs and tighter monitoring, but a fully supervised model doesn’t have to be the most expensive option to score at the top. On the other end, a cheap quiz-and-ship plan is poor value at any price, because it’s missing the safety steps entirely, not discounting them.
Is testosterone safe for the heart, in actual numbers? In the largest trial run to date, major adverse cardiac events occurred in about 7.0 percent of the testosterone group versus 7.3 percent on placebo, a noninferior result that led the FDA to remove its boxed cardiovascular warning and add a caution about blood pressure instead [P3][P6]. The same trial found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism, which is precisely why the follow-up dimension carries weight in this scorecard [P3].
How much of an energy boost should someone realistically expect? Statistically, none that the best available trial could detect. Testosterone showed a real, significant improvement in sexual function and a modest lift in mood, but no significant benefit for vitality [P2]. Worth calibrating expectations around that, especially for anyone whose levels are already in a normal range.
Are TRT clinics legitimate, or are most of them just trying to sell something?
Most clinics built around licensed physicians and state-regulated pharmacies are legitimate, though the depth of care varies a lot between them. The warning signs are the same across the industry: no baseline bloodwork, no required follow-up labs, or pressure toward the most expensive package before you’ve even had your first real conversation. A legitimate clinic treats this as medicine that gets adjusted based on your actual lab results, not a box that ships on a schedule.
How much do TRT clinics typically cost per month?
A realistic range for most fully managed programs is roughly $100 to $300 per month, and that figure moves depending on the delivery method, how often labs are run, and whether insurance is involved at all. Injections generally land toward the lower end, while pellets or specialty gels tend to push costs higher. It’s worth asking every clinic for one all-in number that includes labs, consultations, and medication together, since the advertised entry price rarely reflects what you’ll actually pay monthly.
Which produces better outcomes, telehealth or in-person clinics?
Neither format wins automatically. What actually drives outcomes is how often labs get run, how responsive the clinician is, and whether dosing gets adjusted based on both your numbers and how you actually feel. A telehealth clinic that requires regular bloodwork and gives real clinician access can outperform an in-person clinic that sees you once and then auto-refills indefinitely. The supervision model matters far more than the setting it happens in.
Where should someone actually start when looking for a TRT clinic?
Start with a state medical board website to confirm the clinic’s physicians are actually licensed where you live. From there, compare how each one handles initial bloodwork, follow-up testing, and dose adjustments over time. Compounding-pharmacy-based programs, like the one FormBlends runs, give you a documented, physician-supervised chain of custody for the medication itself. Reading patient reviews that specifically mention follow-up care, rather than just the onboarding experience, tends to tell you more than any single scorecard can.
References
- Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. Bhasin et al., Journal of Clinical Endocrinology & Metabolism, 2018. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Effects of Testosterone Treatment in Older Men (The Testosterone Trials). In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. Snyder et al., New England Journal of Medicine, 2016. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism. Lincoff et al., New England Journal of Medicine, 2023.
- Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism. Wiehle et al., Fertility and Sterility, 2014.
- Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment. Smit et al., F&S Reports, 2025.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added. U.S. Food and Drug Administration.
Written by Dario Ellison, evidence reviewer. Last reviewed May 2026.
Not intended as medical guidance. Speak to a qualified provider about what is right for you.





